
Pheochromocytoma are catecholamine producing tumors derived from the sympathetic or parasympathetic nervous system. The diagnosis of Pheochromocytomas provides a potentially correctable cause of hypertension, and their removal can prevent hypertensive crises that can be lethal.
EPIDEMIOLOGY
Pheochromocytoma is estimated to occur in 2-7 out of 1 million persons per year. The mean age at diagnosis is about 40 years, although the tumors can occur from early childhood until late life. The “Rule of tens” States that about 10% are bilateral, 10% are extra-adrenal, 10% are malignant, 10% are found in asymptomatic patient and 10% are hereditary.
PATHOGENESIS
The name Pheochromocytoma reflects the black coloured staining caused by chromaffin oxidation of catecholamines. A variety of Nomenclature have been used to describe these tumors, but most clinicians use the term Pheochromocytoma to describe symptomatic catecholamine producing tumors.

SIGN & SYMPTOMS
In an earlier studies,blood pressure anomalies were associated with the discovery of Pheochromocytoma in 50% of cases,while headache and palpitations were found in 25% of patients. Pheochromocytoma is typically found with a diverse set of symptoms which may include;
• Anxiety and panic attacks. • Polydypsia. • Polyuria. • Hyperglycemia. • Constipation. • Weight loss. • Visual blurring. • Chest and abdominal pain. • Pallor. • Heat intolerance. • Orthostatic hypotension. • Erythrocytosis. • Tachycardia. • Dilated cardiomyopathy.
DIAGNOSIS
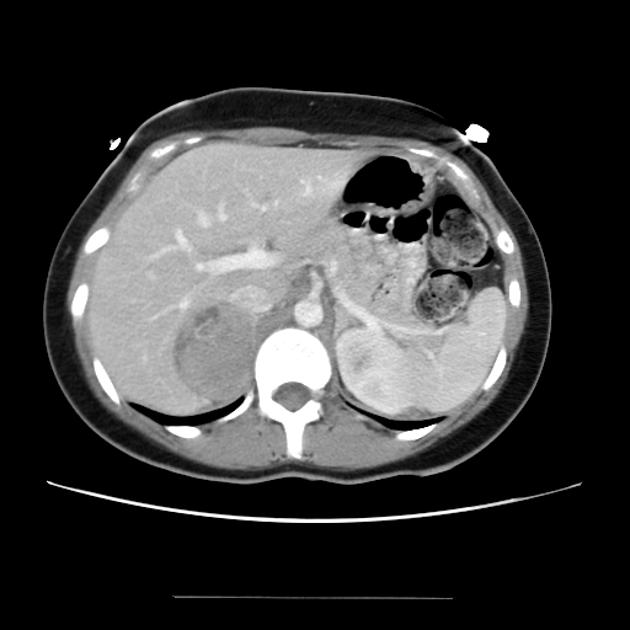
The diagnosis is based on documentation of catecholamine excess by biochemical testing and localization of the tumor by imaging. Both are of equal importance,although measurement of catecholamines is traditionally the first step. High levels of vaniyllylmandelic acid is excreted in urine.
TREATMENT
•Once the diagnosis of a Pheochromocytoma is made,appropriate pre operative medical management is necessary to reduce the risk for peri operative complications. •Complete removal of tumor is the ultimate therapeutic goal. Pre operative patient preparation is essential for safe surgery. Alpha adrenoceptor antagonists,dihydropyridine calcium channel receptor blockers,the tyrosine hydroxylase inhibitor alpha- methyltyrosine, and the competitive alpha & beta receptor blocking drug labetalol have all been successfully used in an oral form for the pre operative treatment. Alpha- adrenergic blockers ( phenotype zamine) should be initiated at relatively low doses (5-10mg po three times per day) and increased as tolerated every few days. Adequate alpha- blockade generally requires 10-14days,with a typical final dose of 20-30mg phenoxybenzamine three times per day. During surgical manipulation of the tumor, massive catecholamine release may occur, which can exceed the normal plasma concentration by > 1000 times. This can result in hypertensive crisis, cardiac arrhythmias, cerebral vascular accident, myocardial infarction or ischemia,pulmonary edema,and multi organ failure.
AIM
The main aim of pharmacological management is to prevent the severe hypotension that can result immediately following removal of the tumor and to abolish or reduce the potentially lethal swings in blood pressure that can occur during induction of an anesthetic and surgical manipulation of the tumor. Stabilization of blood pressure is achieved by the use of a single antihypertensive agent or combination of antihypertensive agents preopertively and intraoperatively to counteract excessive catecholamine adrenergic activity,volume expansion with I.V fluid is achieved, and inotropic support after excision of the Pheochromocytoma if required. There are currently no randomized prospective trials to establish the optimal pre operative pharmacological management of Pheochromocytoma. As a result, there is no clear consensus regarding the drug of choice.

